
News
Meningococcal Vaccination Recommendations for High-Risk Populations: A Cross-Country Review
Invasive Meningococcal Disease (IMD)
Invasive meningococcal disease, or IMD, develops after infection with Neisseria meningitidis. Most of the time, this bacterium simply lives inside a person’s nasopharynx without triggering any noticeable symptoms. Trouble starts when it spreads into the bloodstream or other normally sterile parts of the body. IMD does not occur all that often, but it comes with a high fatality rate and can leave patients with serious long-term health issues.

Looking across the world, serogroups A, B, C, W and Y were once the top causes of meningitis linked to this pathogen. That picture is changing now, though — serogroup X has turned into a major threat throughout Africa. A whole host of factors shape how this disease spreads: where people live, the passage of time, ongoing outbreaks, and differences between groups that face higher exposure. All these variables make it nearly impossible to predict how meningococcal disease will behave in a given area.
Meningococcal vaccines work by stopping infection from the most common disease-causing serogroups. The lineup includes single-strain vaccines for group A (MenA) and group C (MenC), a four-in-one conjugate vaccine covering A, C, W and Y (MenACWY), plus a separate vaccine for serogroup B made with recombinant protein technology (MenB).
Conjugate vaccines built with polysaccharide and protein do more than just shield the people who get the shot. They also cut down on how many people carry the bacteria, lower new infections and slow transmission overall. In turn, folks who did not get vaccinated also gain some level of protection from the community around them.
Health authorities in different countries design local meningococcal vaccination plans mainly for people who are more likely to catch IMD. Risk levels shift with age for the general public. Infants face the greatest danger, followed by young children, teenagers and young adults. In some regions, elderly residents also sit in the high-risk category.
Age is not the only concern. Certain groups deal with elevated risk too: people living with HIV, those who have problems with their complement system, and anyone with a spleen that does not function properly. Even people with no underlying immune problems can end up exposed. College students, indigenous communities, migrant groups, lab staff, military personnel, men who have sex with men, and people traveling to high-risk areas all fall into this category.
A recent piece published in Expert Review of Vaccines took a close look at vaccine guidance for these at-risk populations. The research team put a spotlight on inconsistent advice from one region to another. They compared official recommendations across a wide range of nations — European countries, the United States, Australia, New Zealand, Israel, Brazil and Turkey, to name a few — to spot gaps in vaccine coverage.
These countries were picked for good reasons. They reflect real-world differences in disease burden, run reliable disease monitoring systems, and have long histories with meningococcal vaccination programs. They are also among the first to roll out new vaccines and related medical interventions across the globe.
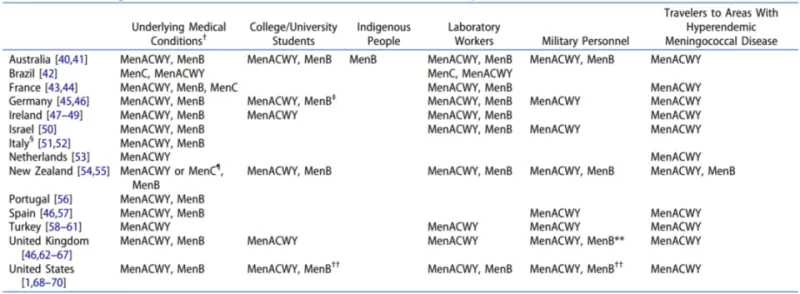
Table 2 Current Meningococcal Vaccine Advice for High-Risk Groups by Country
Notes:
MenACWY = quadrivalent vaccine for meningococcal serogroups A, C, W and Y
MenB = vaccine targeting meningococcal serogroup B
MenC = vaccine targeting meningococcal serogroup C
The guidance listed here is extra advice, separate from standard age-based vaccination rules.
† The term “underlying medical conditions” covers a broad range: cellular immune deficiency, combined immune deficiency, complement disorders, transplant recipients, cancer patients, inherited immune problems and HIV infection are just a few examples. Not every recommendation applies to every condition. Readers should check original official documents for details on specific cases.
‡ Students planning to stay long-term in countries that offer routine teen vaccination or optional school-based shots should get vaccinated ahead of their move. The exact vaccine they need follows local rules in their destination country.
§ The vaccines named here are specified for people without a working spleen. No single meningococcal vaccine is officially marked as the primary choice for patients with other chronic health issues.
¶ Health officials suggest MenACWY (rather than MenC) for high-risk infants younger than nine months old. This recommendation exists, but public funding is not provided for this vaccine group.
Vaccine rules for military members change based on their unit, role and past vaccination history.
†† Health providers may choose to offer MenB to teens and young adults aged 16 to 23 through shared clinical decisions, even though it is not an official required vaccine. People in this age group do not need to have an elevated IMD risk to receive it.
---
Research Scope
Most national and regional immunization programs focus first on groups prone to meningococcal infection. Infants, teenagers, young adults and older adults — the main age-based high-risk groups — are always a top priority. This review expands beyond basic age categories to examine other vulnerable populations.
We look closely at people with weakened immune systems, college students, indigenous communities, laboratory workers, military staff, men who have sex with men, and travelers heading to areas where the disease spreads easily. The core of this work compares local meningococcal vaccine policies for these groups across Europe, the United States, Australia, New Zealand, Israel, Brazil and Turkey.
1. Groups With Medical Risk Factors & Corresponding Guidance
A poorly functioning spleen, disorders within the complement pathway, and HIV infection all drastically raise a person’s chance of contracting meningococcal disease. Patients who have lost their spleen entirely see a fatality rate between 40% and 70% from IMD.
For people born with complement deficiencies, the odds of developing severe invasive meningitis are 1,000 to 10,000 times higher than for average residents. Those living with HIV face a risk roughly ten times greater than the general population. Drugs like eculizumab and ravulizumab, used to treat several chronic illnesses, also put patients at notable risk.
Both long-term immune weakness and certain prescription medications can lower how well vaccines work in the body. Multiple recent reports confirm that people taking complement inhibitors like eculizumab do not gain full protection from standard meningococcal vaccines.
Patients receiving treatment that blocks tumor necrosis factor also show a weaker response after getting the MenACWY conjugate vaccine. Similar reduced immune reactions appear in patients without working spleens and people living with HIV after MenACWY or MenC vaccination. For anyone with a compromised immune system, medical experts suggest giving two primary vaccine doses, or adding booster shots later on.
When it comes to vaccinating people with underlying immune issues, policies differ a lot from country to country. Ireland, New Zealand and Australia advise both MenACWY and MenB for this group. France only recommends MenC vaccines here. Italy suggests using a meningococcal vaccine but does not name a specific type.
In Germany, doctors assess each HIV-positive patient individually to decide whether MenB vaccination is appropriate. Turkey directs immunocompromised patients and HIV-positive children aged 11 to 18 to receive MenACWY. Australia’s national immunization program covers the cost of MenB and MenACWY for people of any age who carry clear risk factors.
Brazil offers MenC and MenACWY to patients with chronic immune conditions. For people with paroxysmal nocturnal hemoglobinuria who take eculizumab, MenACWY is the specifically named vaccine choice.
2. Groups With Elevated Exposure Risk & Corresponding Guidance
(1) University Students
How likely college students are to catch acute meningococcal disease varies widely by region. In the UK and the US, student populations see higher IMD rates, and serogroup B is the main strain behind most cases. In France, most student IMD cases trace back to serogroup W instead.
Unsurprisingly, official advice does not line up across borders either. Health authorities in the US and UK tell college students to get MenACWY. Australia and New Zealand go a step further, recommending both MenACWY and MenB for this group.
Not every nation has set clear, formal rules for student vaccination. Ireland targets first-year secondary school students with MenACWY shots. The goal here is to stop outbreaks from spreading once these students move on to university. While routine MenACWY does cut down overall student risk, the lack of official MenB guidance in many places ties directly to rising serogroup B infections among young people in higher education.
(2) Indigenous Populations
Indigenous communities around the world experience higher rates of invasive meningococcal disease. In Australia, Indigenous people and Torres Strait Islander children — especially those under ten years old — develop serogroup B meningitis far more often than other local groups.
In New Zealand, Māori and Pacific Island residents have a meningitis rate roughly three times higher than people of European descent. Migrants and refugee communities also face increased risk of IMD and other contagious illnesses. Crowded living spaces, poor sanitation and regular exposure to secondhand smoke all add to the danger.
Australia and New Zealand have launched targeted vaccination programs for indigenous groups to shrink these health gaps. None of the other countries reviewed have put dedicated meningococcal vaccine policies in place for their indigenous populations.
(3) Laboratory Workers
Lab professionals who regularly handle meningococcal samples run a much higher risk of developing IMD. Their infection rate stands about 40 times higher than other people in the same age range. Nearly all countries studied recommend meningococcal vaccines for lab staff.
Brazil approves either MenACWY or MenC for this workforce. The UK uses MenACWY as the standard choice. Several other nations require both MenACWY and MenB for lab employees.
(4) Military Personnel
Service members face heightened IMD risk for several reasons. Their age range, constant close contact with fellow troops, and frequent deployments to high-prevalence regions all play a part — much like travelers visiting these same areas.
The US military rolled out routine MenACWY vaccination between 2006 and 2008. After that change, overall IMD numbers across the armed forces dropped. Even so, isolated cases, including fatal ones, still pop up among new recruits from time to time. Most countries classify military staff as high-risk and recommend standard meningococcal vaccines, with strong emphasis placed on MenACWY conjugate shots.
(5) Men Who Have Sex with Men (MSM)
Men who have sex with men carry an increased risk of contracting IMD. One US-based study found that 18% of all recorded IMD cases occurred within this community, with serogroup C as the dominant strain. Local disease outbreaks and co-existing HIV infections are the two biggest drivers pushing case numbers higher here. Major cities across Europe have also recorded rising serogroup C meningitis cases among men who have sex with men.
Vaccine guidance for this group closely follows local outbreak trends. The New York City Department of Health advises all men who have sex with men to get vaccinated against meningitis. The US Centers for Disease Control and Prevention expanded this advice to cover the same community across Florida, recommending MenACWY for everyone in this risk group.
(6) Travelers
People traveling to the so-called African Meningitis Belt, or attending large public gatherings, face greater IMD threats. The recent spread of the W cc-11 strain has only made this risk worse. Back in 2015, more than 33,000 European attendees took part in the World Scout Jamboree held in Japan. Four confirmed cases of serogroup W IMD emerged among this group.
Pilgrims traveling to Mecca in Saudi Arabia for Hajj or Umrah, along with anyone joining large crowds nearby, also see higher infection risk. Meningococcal carriage rates among pilgrims can reach as high as 27%, with exact numbers shifting based on the bacterial serogroup and the traveler’s home country.
Saudi Arabia enforces strict entry rules: anyone aged two or older coming for religious pilgrimages, seasonal workers in pilgrimage zones, and travelers arriving from the African Meningitis Belt must show proof of meningococcal vaccination. Most countries also tell citizens to get vaccinated before traveling to regions with widespread meningitis.
3. Vaccine Uptake & Real-World Implementation
Available data shows that vaccination rates remain low among people with weakened immune systems across multiple regions.
A large retrospective study looking at national US data from 2010 to 2018 tracked patients with anatomical or functional spleen problems (excluding those with sickle cell disease or Crohn’s disease). Only 28.1% received at least one MenACWY dose within three years of their diagnosis, while just 9.7% got at least one MenB shot in that same window.
For patients newly diagnosed with Crohn’s disease over the same period, uptake was even lower: 4.6% received MenACWY and 2.2% received MenB within three years after diagnosis. Among people newly diagnosed with HIV in the US between 2016 and 2018, merely 16.3% got a MenACWY vaccine within two years of finding out their status.
College student vaccination rates also stay relatively low. Rules vary from one college or university to the next across the United States, and this inconsistency directly impacts uptake. Meningococcal vaccines are officially recommended for students nationwide, yet researchers estimate only 53% of US schools actually require the shot.
Among students who do have to get vaccinated, 52% receive MenACWY. Fewer than 1% opt for MenB, which explains in large part why MenB coverage stays so low on college campuses.
In the UK, health officials suggest MenACWY for all university students. A survey carried out at the University of Liverpool polled first-year undergraduates aged 18 to 25 online. The results showed 68% of participating students had received their MenACWY vaccine. In South Australia, publicly funded MenB vaccines reached 77% of 16-year-olds in the region.
This review did not collect specific data on healthcare workers, but existing separate research suggests their vaccination rates follow a similar underwhelming pattern.
Medical professionals hold a key role in educating patients and encouraging them to follow vaccination advice. Even so, many providers do not fully understand current official guidelines. France recommends MenC for everyone between 12 months and 24 years old. A 2016 survey of general practitioners there found fewer than half (under 52%) consistently told eligible patients to get this vaccine.
Other common barriers stand in the way of higher vaccination rates too. Many parents lack basic knowledge about MenC vaccines. A lot of people underestimate how dangerous meningitis can be, and some express doubts about whether vaccines work or worry about potential side effects. Gaps in knowledge among both medical staff and caregivers clearly hold back overall vaccine coverage.
---
Discussion & Analysis
If you compare meningococcal vaccine rules for high-risk groups around the world, the differences are impossible to miss. Australia, Israel, New Zealand, the UK and the US have built fairly broad sets of recommendations. Countries like Brazil, Italy, the Netherlands, Portugal, Spain and Turkey take a much more limited approach.
Choices around vaccine types also do not align globally, especially when it comes to MenB. Some nations stick solely with MenACWY or MenC and do not endorse MenB at all. Several factors create these divides. MenB vaccines arrived on the market later and carry a higher price tag. Many areas also lack robust systems to track local meningococcal activity.
The World Health Organization does not currently advise using MenB for routine mass vaccination of the general population, and this stance influences national policies across many countries as well.
Meningococcal disease progresses extremely quickly. To keep protective antibody levels high in communities worldwide, consistent and long-term vaccine coverage is essential. Unfortunately, countries do not agree on rules for booster shots and repeat vaccinations.
Saudi Arabia enforces strict entry requirements for travelers: visitors must prove they received a MenACWY polysaccharide or conjugate vaccine within the past three to five years, which means regular revaccination is necessary for frequent travelers. Out of all other countries studied, only Australia, Ireland and the US suggest MenACWY boosters for people who face ongoing exposure risk.
Standard booster timelines also vary. Brazil, Ireland, New Zealand and the US recommend a MenACWY booster every five years. New Zealand advises MenB boosters every five years, while the US recommends repeating MenB shots every two to three years.
College students and indigenous communities are well-known high-risk groups, but dedicated vaccine guidance for them remains sparse. Out of the 14 countries reviewed, just six — Australia, Germany, Ireland, New Zealand, the UK and the US — tell college students to get MenACWY.
Outside Australia and New Zealand, almost no countries have routine MenB recommendations for student populations. On a positive note, Italy, New Zealand and Australia have started expanding MenB vaccination programs to cover teenagers and young adults. When it comes to indigenous communities, vaccine advice changes entirely from one country and one community to the next. Updated, targeted policies are needed to address their elevated disease risk.
Vaccine completion rates for high-risk groups leave plenty of room for improvement. Knowledge gaps among medical staff and parents are a major contributing factor. One survey of healthcare workers in Italy found only around one-third fully understood key details: local IMD case numbers and death rates, the most common bacterial serogroups, and which underlying health conditions make severe complications more likely.
In the United States, many clinical staff cannot name the exact rules for different meningococcal vaccines, and interpretations of official guidance vary widely from provider to provider. Better education for medical teams and the general public is critical. People need clear information on IMD risks, available vaccines and local health policies.
---
Expert Perspective
Across all countries included in this research, there is no unified stance on which meningococcal vaccines high-risk groups should receive. To effectively stop IMD, communities need protection against the five main disease-causing serogroups. Even so, not every country offers vaccines that target the strains most active locally.
France, for example, has no clear vaccination guidance for patients with autoimmune disorders, hemophilia or severe chronic respiratory conditions. In the US, serogroup B causes most student IMD cases, yet routine recommendations prioritize MenACWY over MenB. If universal international standards existed, the US would likely follow Australia’s lead and require MenB for all students living on campus.
A number of hurdles stand in the way of global standardization for meningococcal vaccine policies. Different nations have separate rules for vaccine licensing and distribution. Data collection for high-risk and vulnerable groups is often incomplete. Public and professional understanding of meningitis and prevention methods stays low in many regions.
Countries also weigh vaccine cost versus benefits differently, and set different priorities for public health spending. MenB vaccines require multiple doses, which adds another layer of complexity. National immunization schedules are already complex, with multiple primary series and revaccination rules, making uniform global policies harder to put in place.
The new pentavalent MenABCWY vaccine may help resolve some of these issues. This single vaccine protects against all five major serogroups with just two doses. Simplified dosing has the potential to push overall vaccination rates higher around the world.
To move toward more consistent policies and better real-world vaccine use globally, authorities need to improve vaccine access everywhere, build international consensus, and roll out practical plans to boost uptake. The World Health Organization has launched a global roadmap with a clear goal: eliminate meningitis worldwide by 2030.
This plan aims to wipe out epidemic bacterial meningitis through coordinated global policies and vaccination strategies. It works toward direct protection for individuals and community-wide herd immunity wherever possible, cuts down cases and deaths from vaccine-preventable meningitis, and improves quality of life for people who survive severe infection.
Each country will build its own local plans based on regional needs and set priorities that fit local conditions. Other international organizations can also step in to help align meningococcal vaccine guidance across borders.
---
Conclusion
Official vaccination advice for people at high risk of invasive meningococcal disease differs drastically across the globe. Major inconsistencies exist between policies for MenB, MenACWY and MenC vaccines. In many cases, national guidelines do not even match up with the bacterial serogroups causing most local infections.
Updating and unifying global vaccination rules for the five main meningococcal serogroups is vital to protect vulnerable populations. Revised guidance should expand coverage to include every high-risk group. Policymakers must account for which serogroups circulate locally and all unique regional risk factors.
Alongside updated rules, practical strategies to raise vaccination rates are necessary. Adding structured booster shot schedules will also help maintain long-term protection against this dangerous disease.
Related News
- Why Is the Y-Type Meningitis Vaccine Important for Long-Term Protection Against Meningococcal Disease?
- Meningococcal Vaccine Guide
- Why Is Meningococcal Polysaccharide Vaccine Essential for Protecting Against Serious Meningococcal Disease?
- Why Is the Meningitis Vaccine So Important for Protection?
- Why Is Hepatitis A Vaccine for Prevention Essential for Long-Term Health Protection?
- Why Is Children Hepatitis A Vaccine Important for Kids’ Health?
Leave me a message








")


